Laser safety management (medical and cosmetic applications)
'Core of knowledge' course notes
Hazards and risks
We will define a HAZARD as, something that can cause harm.
And RISK as, the probability of the hazard causing harm and the severity of that harm.
For example the laser/IPL machine is the hazard and the risk is the likely-hood of damage to the eye and skin from the light emitted from these machines.
Risk to the skin
Relatively speaking this is not usually a significant hazard to the operator, because the damage is likely to be superficial and will probably heal in time. However, in the case of medical and cosmetic lasers, treatments often entail deliberately exposing a patient's skin to intense optical radiation. If the treatment is performed incorrectly, the skin can be severely burned. Whilst burns will typically be superficial, they can look fairly dramatic and be very distressing for the patient.
Risk to the eye
The eye is at particular risk for the following reasons:
- Damage to the retina (back of the eye) is likely to be irreparable
- Damage can occur at large distances from the laser aperture
- Damage can occur from exposure to very low power lasers
- Even reflections can be hazardous
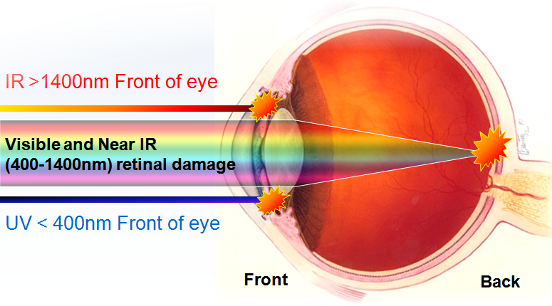
The area of the eye that is susceptible to damage is dependent on the wavelength of the laser or intense light source.
Retinal damage (back of the eye)
Exposure to visible and near infra red light can cause permanent blindness.
Even light of relatively low energy can be a hazard to the retina. This is because the lens of the eye focuses light onto a very small point at the back of the eye which greatly increases the intensity. Low power lasers of even a milliwatt can be dangerous.
Only a fraction of the energy is directly absorbed by rods and cones, the remainder being absorbed by melanin in the epithelium. This causes local heating and hence indirect damage to adjacent rods and cones.
If sufficiently intense, this may result in permanent loss of vision, which will be noted by the subject only if the macula is involved. This is likely to occur if the subject was looking directly at the beam. Peripheral loss will only be noted with gross damage or maybe by an ophthalmic examination.
Anterior (front of eye) damage
Very short (less than 315 nm) and very long (more than 1400 nm) wavelengths are absorbed in the cornea. If the damage is superficial and limited to outer layers, then the cornea will repair itself due to fast turnover of surface cells. Some wavelengths (315 to 400 nm and 760 to 1400 nm) will deposit some of their energy in the lens of the eye. This could lead to cataract formation if the energy is sufficiently high.

Risk Perception
With 'normal' white light sources, the brightness we perceive broadly relates to the risk the source presents. However, with laser light we cannot always judge the hazard visually. For example, laser light in the region 700-1400nm is invisible, yet even low levels can cause damage to the retina of the eye. In addition, our vision is relatively sensitive to green light, so we might be naturally cautious of a green laser. However, a red or violet laser beam would appear dull by comparison but present a very similar risk to the eye.
Non-Beam Hazards
As well as the direct risk from the intense light beam to the eyes and skin, the use of laser/IPL equipment may pose other dangers to staff, patients/clients and members of the public.
Laser Generated Airborne Contaminants (Laser Plume)
When target tissue exposed to the air is 'lased', a huge number of vaporised human cells are ejected into the air. It is thought that some biological matter may still be viable and pose a health risk to all those present.
High Voltage
Access to high voltage (HV) is normally via special panels. Any faults with the machine should only be rectified by trained staff. In particular it should be noted that with some lasers the capacitors remain charged for a considerable period, even after the laser has been switched off, and are capable of delivering a lethal shock.
Fire risk
Many lasers are capable of setting fire to flammable materials and represent a fire risk.
Anaesthetic gases
This is a potential problem, especially in ENT surgery, since the beam is very close to the anaesthetic tube. Special laser proof tubes are available to mitigate against this.
Cross-infection
As with any medical and cosmetic procedure, the risks of cross infection should be considered.
Chemicals
Some lasers (e.g. dye/excimer) use toxic liquids and gases which can even be fatal even at low concentrations.
Slips trips and falls
Trailing wires are a common example of this type of hazard.
Personal security
Consideration should be given to the fact that the operator may be in a closed room alone with the client/patient.
Who is at risk
It is sometimes helpful to broadly categorise the various 'at risk groups'. These may include:
- Staff: Operators, Any other assisting staff present in the hazard area, Other staff who may enter the laser hazard area by accident.
- Patients / Clients
- Members of the public
Risk Assessment (medical, cosmetic, dental applications)
The risk assessment is a process designed to identify any hazards, quantify the risks from those hazards and look at appropriate safety controls that may need to be put in place. The risk posed by the laser will vary depending upon a number of factors such as;
a) Wavelength of the laser,
b) Output of the laser (maximum power or energy),
c) How the laser is used (e.g. inside the patient or free-hand.
In essence we will want to find out if it is possible to be exposed to a laser beam of sufficient intensity to cause damage (to the eye or skin). We then would decide if there is a reasonable probability of this happening.
Safe Distance
Since medical and cosmetic lasers are usually designed to have some effect on the human body, it is reasonable to assume that, at source, the beam will exceed the safe intensity (known as the Maximum Permissible Exposure) and will present a hazard.
However, the beam will then diverge to some extent and at some point the intensity will be low enough for the beam to become safe. The distance at which this happens is known as the Nominal Ocular Hazard distance (NOHD).
This hazard distance can be calculated if factors such as the output, divergence and aperture size are known. However, with modern medical laser equipment, this information can usually be obtained from the equipment supplier/manufacturer and is often listed in the user manual.
Knowing the hazard distance will help us decide whether certain controls are needed to ensure the laser light does not escape the confines of the area. Window coverings may be needed if the NOHD is larger than the room dimensions for example. It is not absolutely necessary the NOHD however. In practice, many people just assume the NOHD exceeds the room dimensions as this allows any laser to be used in the facility (without costly retrofitting blinds etc.) and enables a 'standard' set of procedures to be followed.
Protective eyewear (laser)
Assuming protective eyewear will be needed (as it usually is), we will also need to know what level of protection is needed. Historically, this is usually taken to be the level of attenuation needed to make the laser 'safe' at a distance of 0.1m from the beam and is expressed as an 'optical density'. Again, the eyewear specification will almost certainly be described in the equipment manual.
Sources of initial information?
Details such as equipment specification, hazard distance and eyewear specification can be obtained from a number of sources;
a) Safety adviser (e.g. laser protection adviser),
b) Equipment supplier,
c) Equipment manufacturer,
d) User manual and training materials,
e) Equipment labels.
Who can carry out the risk assessment?
Any competent person can lead the risk assessment process. However, we usually to refer to the 'risk assessment team'. This may include;
a) Safety adviser (e.g. laser protection adviser),
b) Laser operator(s),
c) Facility manager.
Documenting the risk assessment?
In UK law, the significant findings of the risk assessment must be documented if the business employs five or more people. It is generally recommended that the risk assessment is documented regardless though, as otherwise there may be no evidence that a risk assessment has actually been done.
Course resource  Risk assessment example template form and guidance Risk assessment example template form and guidance |
When should the risk assessment be revisited?
The risk assessment must be reviewed;
a) Following any significant changes,
b) If it is suspected that the controls are not adequate (e.g. following an incident),
c) Any relevant chanages in safety law.
It is also useful to review the assessment,
d) Periodically (e.g. annually).
|
Revision Questions 1. Why is laser light in the region 400-1400nm particularly dangerous? 2. What do we mean when we say we can't judge the laser hazard visually? 3. What do we mean by 'non beam' hazards? |


