Laser Safety Management for
Medical Applications
Light fundamentals
Light is a form of energy and when talking about safety, we sometimes refer to it as optical radiation. It can be described as rays, particles or waves. For our purposes, describing light as waves will be the most helpful.
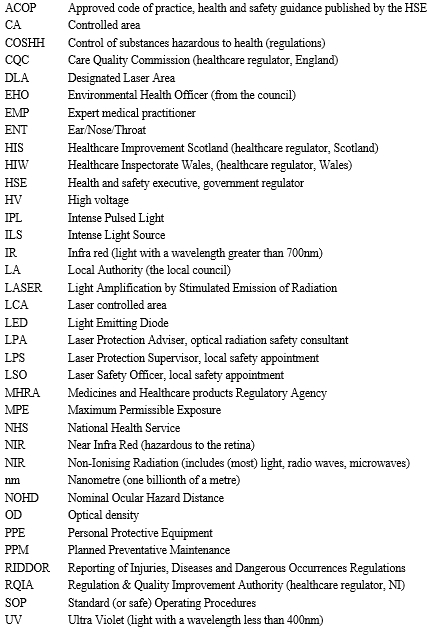
For light, the wavelength defines the colour and is summarised in the table below. 1nm = 1,000,000,000th of a metre.
It is useful to know the wavelength for the following reasons;
- Indication of the hazard/risk
- Calculating the damage threshold (eyes and soft tissue)
- Determining whether a laser beam is visible or invisible
- Protective eyewear selection

Lasers and IPLs - physical characteristics
Laser light
Laser light is a typically an intense beam of optical radiation. It is different from all other light sources in the way it is generated. Typically laser light exhibits the following properties:
- Single colour (monochromatic)
- Collimated (non divergent)
The second property can be seen in the example of a laser pointer. The size of the spot does not spread out in the same way the light from a traditional handheld torch would. This unique property means that whilst the power of a laser may one hundred times lower than a household light-bulb, the beam can be hazardous at a distance of hundreds of meters away from the source.
Lasers are typically named according to their laser medium. This is the material that sits inside a cavity in a laser machine where the laser light is generated. Each laser medium emits light of a characteristic wavelength.
Some examples of medical and cosmetic lasers are listed below.
Carbon Dioxide
The laser medium in this case is a gas. The laser light produced is in the far infra red region (10600 nm)
Nd:YAG
The Neodymium: Yttrium Aluminium Garnet laser is 'solid state' in that it does not use a gas but rather a crystal as the lasing medium. It produces 1064 nm wavelength light (near infrared) which is invisible. A crystal can also be used to 'half the wavelength' to 532nm (green).
Excimer
The excimer laser uses an 'excited dimer' lasing medium. For example the Argon Fluoride (ArF) emits in the UV region (193 nm) and is used in corneal sculpturing (laser eye surgery).
Solid State (diode)
This is a special form of light emitting diode, familiar on electronic equipment. They are very efficient (up to 50%) so that little cooling is required. Wavelengths from 630 - 2100 nm are available.
Intense Pulsed Light (IPL)
IPL (intense pulsed light) devices are also known as IPLS (intense pulsed light sources), full spectrum, non-coherent, and broadband light. These devices are a newer innovation in the cosmetic industry and emit light that has slightly different properties to a laser beam:
- Not monochromatic (broad spectrum)
- Generally more divergent
However, since these devices are capable of delivering very intense bursts of light they usually incur similar safety precautions as lasers.
Uses of IPLs include hair removal, acne treatment, skin rejuvenation and other cosmetic procedures. Due to the broad spectrum of light, filters can be used to select specific portions of this spectrum enabling a range of treatments to be undertaken with the same machine.
Light is generated in a very different way to laser light. Typically a Xenon Flash Lamp is used. This is basically a glass tube filled with Xenon gas. A large current is pulsed through the gas which energises the xenon atoms which promptly de-excite (spontaneous emission) to give of light photons.
Light is actually given off at a variety of discrete wavelengths. However, these are sufficiently spaced out over the visible spectrum that to the human eye the output appears to be a white light. Filters are used to alter the output spectrum at the point of treatment.

IPL treatment handpiece and filter set
Difference between Laser and other therapeutic intense light sources
Whilst the therapeutic effects of Laser light and light from an IPL device can be very similar, the way the light is generated is very different. A comparison between the properties of the light is given below.
Laser light = single colour (monochromatic)
IPL = broad spectrum (polychromatic)
Laser light = can be collimated so that it does not diverge for hundreds of meters
IPL = diverges very quickly
Laser light = can be operated continuously or pulsed
IPL = operated in pulses (in the case of a Xenon lamp)
Biological interaction
When intense light from a laser or other intense source of sufficient energy is direction onto the tissues of the body, the effect varies depending upon the timescale with which the energy is delivered. This can be broadly categorised under three headings.
Photo-mechanical and Acoustic effects (less than microseconds)
Energy is deposited as a shock wave and results in physical disruption and cell rupture, in a short period of time - the effect is very localised. The technique is used in Ophthalmology, Lithotripsy (for the fragmentation of stones in situ) and for tattoo removal.
Thermal effects (less than milliseconds to several seconds)
The energy is absorbed by cell molecules. This leads to an increase in temperature of the cell and adjoining cells which show burn characteristics and tissue damage due to protein denaturation (above 60C). Above 100C the tissue vaporises and at about 350C burns. This is the most common effect used in medicine and is used for thermal shrinkage (sealing small blood vessels) or for tumor removal (either by surgical cutting or total ablation of tissue). Most hair reduction techniques also make use of thermal effects.
Photochemical effects (greater than several seconds)
Low level intensity light is used to activate the cell or administered chemical molecules. The response is very wavelength dependent and is used in Physiotherapy lasers and for Photodynamic Therapy. The effect can result from a single long exposure or multiple short exposures.
Wavelength and transmission through tissue
The depth to which light will penetrate tissue depends on its wavelength. At extreme wavelengths (short ultraviolet and long infra-red) all of the energy is absorbed by the surface cells, and so there is no penetration. Hence the CO2 laser is used for debulking tissue (tumor removal), since almost all of its energy is absorbed within the first 0.2 mm. In contrast the visible and Nd:YAG lasers penetrate to a greater depth (0.5 to 2 mm) on the skin and will not be absorbed (significantly) by the cornea and lens of the eye. Hence their used in dermatology, ophthalmology and cosmetic treatments such as hair reduction.
![]()
Relative penetration of light into the skin
|
Revision Questions 1. Put simply, what property of light does wavelength define? 2. How does laser light differ from 'normal' light? 3. Why is is useful to know the wavelength? |
Hazards and risks
We will define a HAZARD as, something that can cause harm.
And RISK as, the probability of the hazard causing harm and the severity of that harm.
For example the laser/IPL machine is the hazard and the risk is the likely-hood of damage to the eye and skin from the light emitted from these machines.
Risk to the skin
Relatively speaking this is not usually a significant hazard to the operator, because the damage is likely to be superficial and will probably heal in time. However, in the case of medical and cosmetic lasers, treatments often entail deliberately exposing a patient's skin to intense optical radiation. If the treatment is performed incorrectly, the skin can be severely burned. Whilst burns will typically be superficial, they can look fairly dramatic and be very distressing for the patient.
Risk to the eye
The eye is at particular risk for the following reasons:
- Damage to the retina (back of the eye) is likely to be irreparable
- Damage can occur at large distances from the laser aperture
- Damage can occur from exposure to very low power lasers
- Even reflections can be hazardous
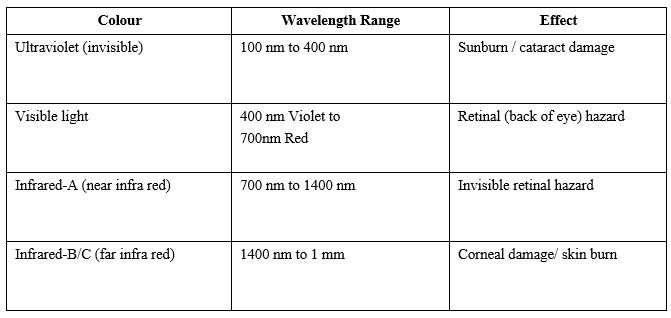
The area of the eye that is susceptible to damage is dependent on the wavelength of the laser or intense light source.
Retinal damage (back of the eye)
Exposure to visible and near infra red light can cause permanent blindness.
Even light of relatively low energy can be a hazard to the retina. This is because the lens of the eye focuses light onto a very small point at the back of the eye which greatly increases the intensity. Low power lasers of even a milliwatt can be dangerous.
Only a fraction of the energy is directly absorbed by rods and cones, the remainder being absorbed by melanin in the epithelium. This causes local heating and hence indirect damage to adjacent rods and cones.
If sufficiently intense, this may result in permanent loss of vision, which will be noted by the subject only if the macula is involved. This is likely to occur if the subject was looking directly at the beam. Peripheral loss will only be noted with gross damage or maybe by an ophthalmic examination.
Anterior (front of eye) damage
Very short (less than 315 nm) and very long (more than 1400 nm) wavelengths are absorbed in the cornea. If the damage is superficial and limited to outer layers, then the cornea will repair itself due to fast turnover of surface cells. Some wavelengths (315 to 400 nm and 760 to 1400 nm) will deposit some of their energy in the lens of the eye. This could lead to cataract formation if the energy is sufficiently high.

Risk Perception
With 'normal' white light sources, the brightness we perceive broadly relates to the risk the source presents. However, with laser light we cannot always judge the hazard visually. For example, laser light in the region 700-1400nm is invisible, yet even low levels can cause damage to the retina of the eye. In addition, our vision is relatively sensitive to green light, so we might be naturally cautious of a green laser. However, a red or violet laser beam would appear dull by comparison but present a very similar risk to the eye.
Non-Beam Hazards
As well as the direct risk from the intense light beam to the eyes and skin, the use of laser/IPL equipment may pose other dangers to staff, patients/clients and members of the public.
Laser Generated Airborne Contaminants (Laser Plume)
When target tissue exposed to the air is 'lased', a huge number of vaporised human cells are ejected into the air. It is thought that some biological matter may still be viable and pose a health risk to all those present.
High Voltage
Access to high voltage (HV) is normally via special panels. Any faults with the machine should only be rectified by trained staff. In particular it should be noted that with some lasers the capacitors remain charged for a considerable period, even after the laser has been switched off, and are capable of delivering a lethal shock.
Fire risk
Many lasers are capable of setting fire to flammable materials and represent a fire risk.
Anaesthetic gases
This is a potential problem, especially in ENT surgery, since the beam is very close to the anaesthetic tube. Special laser proof tubes are available to mitigate against this.
Cross-infection
As with any medical and cosmetic procedure, the risks of cross infection should be considered.
Chemicals
Some lasers (e.g. dye/excimer) use toxic liquids and gases which can even be fatal even at low concentrations.
Slips trips and falls
Trailing wires are a common example of this type of hazard.
Personal security
Consideration should be given to the fact that the operator may be in a closed room alone with the client/patient.
Who is at risk
It is sometimes helpful to broadly categorise the various 'at risk groups'. These may include:
- Staff: Operators, Any other assisting staff present in the hazard area, Other staff who may enter the laser hazard area by accident.
- Patients / Clients
- Members of the public
Risk Assessment (medical, cosmetic, dental applications)
The risk assessment is a process designed to identify any hazards, quantify the risks from those hazards and look at appropriate safety controls that may need to be put in place. The risk posed by the laser will vary depending upon a number of factors such as;
a) Wavelength of the laser,
b) Output of the laser (maximum power or energy),
c) How the laser is used (e.g. inside the patient or free-hand.
In essence we will want to find out if it is possible to be exposed to a laser beam of sufficient intensity to cause damage (to the eye or skin). We then would decide if there is a reasonable probability of this happening.
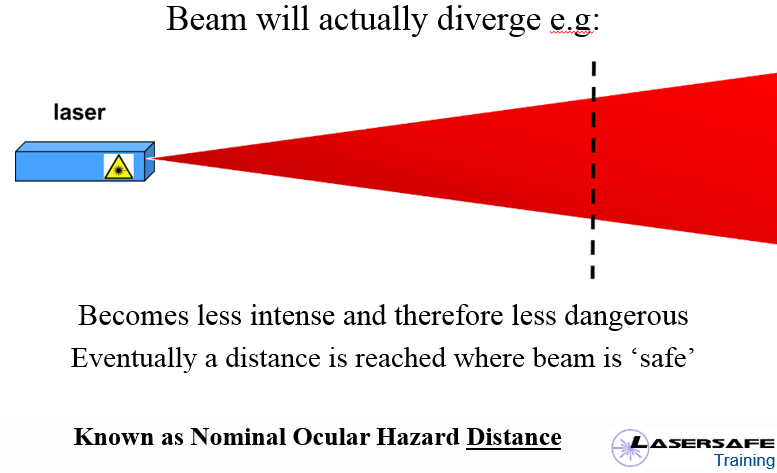
Safe Distance
Since medical and cosmetic lasers are usually designed to have some effect on the human body, it is reasonable to assume that, at source, the beam will exceed the safe intensity (known as the Maximum Permissible Exposure) and will present a hazard.
However, the beam will then diverge to some extent and at some point the intensity will be low enough for the beam to become safe. The distance at which this happens is known as the Nominal Ocular Hazard distance (NOHD).
This hazard distance can be calculated if factors such as the output, divergence and aperture size are known. However, with modern medical laser equipment, this information can usually be obtained from the equipment supplier/manufacturer and is often listed in the user manual.
Knowing the hazard distance will help us decide whether certain controls are needed to ensure the laser light does not escape the confines of the area. Window coverings may be needed if the NOHD is larger than the room dimensions for example. It is not absolutely necessary the NOHD however. In practice, many people just assume the NOHD exceeds the room dimensions as this allows any laser to be used in the facility (without costly retrofitting blinds etc.) and enables a 'standard' set of procedures to be followed.
Protective eyewear (laser)
Assuming protective eyewear will be needed (as it usually is), we will also need to know what level of protection is needed. Historically, this is usually taken to be the level of attenuation needed to make the laser 'safe' at a distance of 0.1m from the beam and is expressed as an 'optical density'. Again, the eyewear specification will almost certainly be described in the equipment manual.
Sources of initial information?
Details such as equipment specification, hazard distance and eyewear specification can be obtained from a number of sources;
a) Safety adviser (e.g. laser protection adviser),
b) Equipment supplier,
c) Equipment manufacturer,
d) User manual and training materials,
e) Equipment labels.
Who can carry out the risk assessment?
Any competent person can lead the risk assessment process. However, we usually to refer to the 'risk assessment team'. This may include;
a) Safety adviser (e.g. laser protection adviser),
b) Laser operator(s),
c) Facility manager.
Documenting the risk assessment?
In UK law, the significant findings of the risk assessment must be documented if the business employs five or more people. It is generally recommended that the risk assessment is documented regardless though, as otherwise there may be no evidence that a risk assessment has actually been done.
When should the risk assessment be revisited?
The risk assessment should undergo review;
a) Periodically,
b) Following any significant changes,
c) Following any incident.
|
Revision Questions 1. Why is laser light in the region 400-1400nm particularly dangerous? 2. What do we mean when we say we can't judge the laser hazard visually? 3. What do we mean by 'non beam' hazards? |
Safety Controls
The risk assessment will determine the most appropriate controls to effectively manage the risks from intense light. Examples of typical controls are listed below.
 Written policies and procedures
Written policies and procedures
Written procedures form part of the training system and help ensure consistent working practices.
Designation of a "controlled area"
The 'controlled area' is the area in which it is possible for intense light to cause harm. In medical and cosmetic applications, it is typical to designate the treatment room or theatre as a controlled area. Note that this only applies when the hazard is present (i.e. the machine is on). Many of the controls below are introduced to,
a) Manage the risks to the operators and patient/clients in the controlled area
b) Prevent harmful levels of light escaping the controlled area
c) Prevent unauthorised access to the controlled area
Design features of the machine
Design features of the machine may only allow exposure in certain directions for example, or when the laser device is in contact with the skin. Other features may include a key (or pin) control to prevent unauthorised access, shielded fibres, shielded foot-switches and emergency stops.
Training and instruction
Trained competent staff are absolutely vital and also a legal requirement. The provision of training and instruction can be achieved in a number of ways and typically include;
- Applications training (how to use the machines and perform treatments): This is typically achieved by practical 'hands-on' training, backed up with written instructions.
- Safety training: Typically achieved through safety briefs/talks and written instructions ("local rules", see below).
Workplace culture
Maintaining a good health and safety 'culture' in the workplace is important.
Safe working practices
Again, established safe working practices and clear policies and procedures are an effective control.
Measures to confine the light to the room
May include blinds/covers on windows, addressing double door gaps etc.
Warning signs
Placed at the entrances to a defined area, these deter unauthorised entry. Illuminated signs can also be connected to the laser power supply, which activate automatically when the laser is in use.
See also: Laser/IPL warning signs examples and information

Example of illuminated warning signs. Note the difficulty in positioning these at eye level.
Plume controls
These may include; 'Smoke' evacuators and face masks. The term 'plume' or 'Laser generated airborne contaminants (LGAC)' is sometimes used.
Personal protective equipment (PPE)
Eyewear, gloves and face masks.
Control of access
Controls may include, warning signs, barriers, door interlocks etc. Consideration may be given to locking of the treatment room doors.
Reflections
The vast majority of medical and cosmetic lasers are 'Class 4', meaning that even reflections from rough/matte surfaces are potentially hazardous. We therefore often treat every surface in the room as if it were a mirrored surface and control exposure to the beam through administrative procedures and eyewear.
We would generally recommend the removal of any reflective surface which may further concentrate the intensity of the beam or increase it's Nominal Ocular Hazard Distance (NOHD). In practice, reflective objects of this design are rare.
The above statement is sometimes misinterpreted as simply "reflective surfaces", which causes confusion over light fittings and chrome door handles etc. It also may lead people to assume that only reflections from mirrored surfaces are hazardous.
Eyewear
Whilst most industrial users of lasers manage to enclose laser beams, medical and cosmetic laser users almost always have to resort to protective eyewear.
Eyewear should be:
- CE marked
- In a good state of repair
- Stored correctly
- Kept clean and hygienic
- Offer an appropriate level of attenuation at the appropriate wavelength(s)
It is a legal requirement that staff should be trained in the correct use of the eyewear. Typically, eyewear labelling is not user friendly and this carries a significant risk of using the wrong type.
For patient/client use, fully opaque shields are available. These should be used for treatments close to the face.
See: patient/client eye-protection
Laser Eyewear
Laser eyewear is wavelength specific. It is therefore very important that firstly, the correct eyewear is obtained and secondly, where different lasers are used, measures are taken to prevent accidentally using the wrong ones. These measures may include extra labeling and separate storage. Staff training should feature in these controls.
Visibility with laser eyewear is often good, as only a small part of the visible spectrum needs to be blocked out.
It is accepted practice to also protect the eyes of unconscious patients as the eye-lid alone is not generally accepted as a suitable laser barrier.
Laser eyewear is usually tested to a relevant safety standard (EN 207 in Europe, ANSI Z136 for the US).
Intense Pulsed Light (IPL) Broadband Eyewear
IPL eyewear is potentially problematic. This is because the equipment emits light over a broad spectrum and blocking against all visible light impairs vision (similar to wearing sunglasses indoors).
Whilst safety standards do exist for IPL eyewear (e.g. EN 8497: 2008), the vast majority of eyewear supplied in Europe and the USA, seems to use the welding shade scale. Typically,
- Welding Shade 3 (typically light green) are provided for the operator.
- Welding Shade 5 (typically dark green) are provided for clients for treatments away from the face.
These do not offer anywhere near the attenuation of laser goggles (which often reduce the laser light by a millionth!) and instead block out the light to the same degree as dark sunglasses (~60%).
'Automatic shields' are also available which offer normal vision but are equipped with a fast acting 'shutter' against bright light from IPL equipment.
The visibility problem and lack of suitably specified eyewear means that the issue of personal protective equipment for IPL devices is less than ideal.
It is worth mentioning that due to the highly divergent nature of the light from an IPL device, reflections will not generally be a problem, as the IPL head would probably have to be pointed straight at the eye to cause damage. However, there is usually a fair amount of 'leakage' from the sides of the crystal which can be unpleasant for those operating the device over a long period.
Warning signs
Whilst it is unlikely that someone entering a room where laser treatments are being carried out will receive an eye strike (lasers are either directed onto or inside the patient), unauthorised entry could cause a distraction to the laser operator who could make a mistake. Ideally, signs should be displayed at eye level.
Signs affixed to treatment room door. This is not ideal as the hazard is not present all the time.
Illuminated warning signs are commonly used in hospitals as these can be wired so as to light up when the laser is switched on. Modern illuminated warning signs tend to use LED which largely removes the requirement to constantly check bulbs for failure.
A common mistake is to permanently display signs stating words to the effect of "laser, do not enter". Treatment rooms are only designated as a "controlled area" whilst a laser/IPL session is underway. Signs should be removed when the machine is not being used. However, for rooms where the machines are more or less in constant use, the examples below could be used.


See: Laser/IPL warning signs examples and information
In cases where eyewear is stored outside the room, blue "eyewear must be worn" signs can be displayed on the outside of the entrance. However, this situation is rare in a medical/cosmetic environment and so there is usually no need to display this sign.
Under the UK Health and Safety (Safety Signs and Signals) Regulations 1996, the following is required:
- Signs are maintained in good condition
- Comprehensible and relevant information on the measures to be taken in connection with safety signs is provided to employees.
- Employees receive suitable and sufficient instruction and training in the meaning of safety signs and the measures to be taken in connection with safety signs.
- The effectiveness of a sign must not be adversely affected by placing of too many signs too close together.
Written Safety Procedures (Local Rules)
The term "Local rules" is sometimes used to describe general procedures for the safe use of laser and other intense light equipment. They typically include information such as,
- Description of the hazard
- Definition of a designated working area
- Key contacts/personnel
- Key safety instructions
- Correct use of Personal Protective Equipment (PPE)
- Meaning of signage
- Emergency procedures
- Refer to specific operating procedures for the actual activity
Some general tips are given below for anyone writing a 'local rules' document.
1. Identify the target readership and the key safety points you want them to take on board.
2. Where possible, aim to cover all rooms and lasers into a single concise document.
3. In the same way, aim to standardise the controls. For example whilst it isn't strictly necessary to cover windows for CO2 lasers, it may be less confusing to include this as a universal control.
4. Ensure that understanding is checked rather than ask staff to just read and sign.
5. Use plain English and avoid specialist terminology and acronyms as much as possible.
|
Revision Questions 1. Why are 'engineering controls' preferable to administrative controls and PPE? 2. What practical controls might you take to help reduce the risk of mixing up the eyewear? 3. Why is it difficult to protect against broad spectrum light sources (e.g. IPL) with eyewear? |
Maximum permissible exposure
Various exposure data has been analysed and international safety committees have been able to publish levels of intense light above which it is deemed that harm will occur.
The Maximum Permissible Exposure (MPE) is defined as,
The level of optical radiation to which, under normal circumstances, persons may be exposed without suffering effects.
The MPE varies depending upon;
a) Wavelength of light
b) Duration of exposure
c) Beam intensity
d) Target tissue (eye or skin)
MPE figures are typically given in terms of energy or power density.
Hazard Distance
All light sources spread out as they propagate away from their origin. At a certain distance the intensity of the light will not be strong enough to cause damage to the eye. This distance is known as the Nominal Ocular Hazard Distance (NOHD).
A technical definition of the NOHD is,
The Minimum distance from the light source at which the exposure to the beam falls below the Maximum Permissible Exposure (MPE)
This is useful when determining the safety controls of a particular facility. It may be of the order of a few centimetres (physiotherapy lasers) or tens of meters. It is mainly determined by the divergence of the beam but wavelength, duration of exposure and output power all have an effect.
Light from an IPL spreads out quickly. In theory, the hazard distance should be relatively short. However, in the absence of manufacturer data, we can often just assume the worst case of "greater than room dimensions".
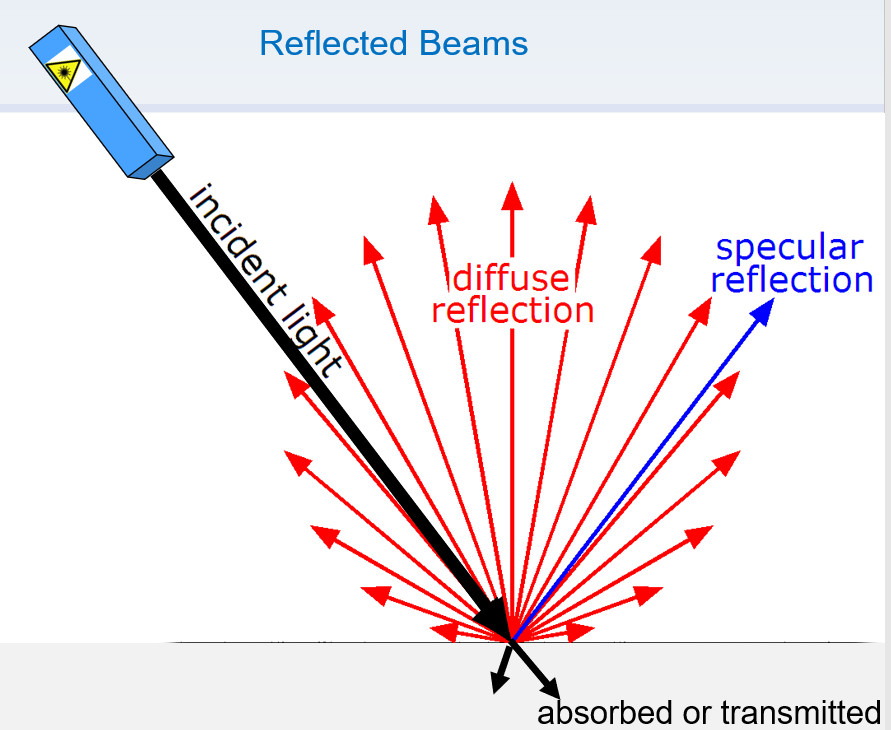
When the laser beam hits an object, a number of things will happen. These include;
- absorption of laser engery into the material
- transmission of some light through the object (if not opaque)
- Specular reflection (e.g. mirror-like reflection)
- Diffuse reflection, e.g. from rough/matte surfaces.
We may be able to estimate the amount of reflected or absorbed light for risk assessment pourposes. In some cases, we may be able to assume a signifcant amount of absorption as the reflectance of dead-flat (no gloss/sheen) painted surfaces can be less than 1%. We may also be able to assume a fully diffuse (Lambertian) refelection.
|
Revision Questions 1. Which wavelengths (colours) are most dangerous to the eye (see page 2)? 2. Would you expect the MPE to be relatively lower or higher at these wavelengths? 3. Why is useful to know the 'hazard distance'? |
European Safety Standards
There are many European standards applicable to those using laser and IPL equipment. The most relevant ones are listed below.
Laser equipment
BS EN 60825, Safety of laser products, IEC 2014
This document contains values for "maximum permissible exposures" (MPE) for the eye and skin. Exposure to laser light above these values will result in harm. Worked examples of Nominal Ocular Hazard Distance (NOHD) are also included in this standard.
The laser classification system is also introduced here. There are several "classes" of laser ranging from class 1 (safe, e.g. laser in CD player) to class 3B and 4 (used for medical and cosmetic therapy).
Class 3B laser product
- normally hazardous for direct beam exposure
- viewing diffuse reflections is normally safe
- output lower than 500mW
Class 4 laser product
- can produce hazardous diffuse reflections
- may cause skin injury
- potential fire hazard
Class 3B and Class 4 lasers (the ones used for most medical and cosmetic treatments) represent a significant risk to the eye and skin.
Class 1C laser product
Introduced in 2014, this is any laser product which is designed explicitly for contact application to the skin. The laser may be as powerful as those mentioned above, but the product is sufficiently well designed to ensure that during operation, the eye hazard is prevented by engineering means. This might apply to a laser device intended for hair removal, where sensors at the laser 'head' prevent operation unless direct contact with the skin is maintained.
IPL equipment
BS EN 60601-2-57:2011 Medical electrical equipment part 2-57 particular requirements for the basic safety and essential performance of non-laser light source equipment
This is a relatively new standard and introduces a classification system for IPL devices.
The classification ranges from "exempt" to "RISK GROUP 3" which pretty much all IPL devices used for treatments such as hair removal fall into. Risk Group 3 devices represent a significant hazard to the eye or skin. Standard warning labels and safety instructions are also described in this document.
Eyewear standards
Standards also exist for safety eyewear:
- BS EN 207 and BS EN 208 for laser eyewear
- BS EN 8497-1 for IPL eyewear.
The laser standard can be confusing for the layman and has even been described as counterproductive. However, it does at least guarantee some level of quality and assurance for the user.
The IPL eyewear standard has so far gone largely ignored as suppliers have already invested in eyewear conforming to generic standards or "welding" eyewear standards.
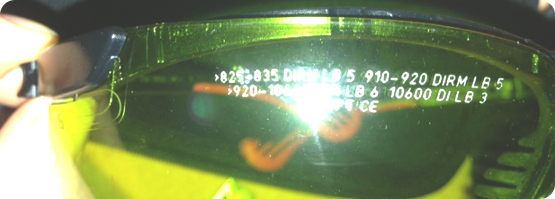
Basic guide to understanding eyewear markings (BS EN 207)
Traditionally, laser eyewear was defined by the following,
- Wavelength or wavelength range the eyewear filters were suitable for
- The amount of attenuation they offered, stated as Optical Density (OD)*
- Visible light transmission (VLT), level to which they block all ambient light
*Optical density is a logarithmic scale, i.e.
OD 1 attenuates light by 10 times
OD 2 attenuates light by 100 times
OD 3 attenuates light by 1000 times and so on.
However, this does not take into account the capability of the laser beam to physically damage the eyewear. To address this, scale numbers were introduced in the 207 standard.
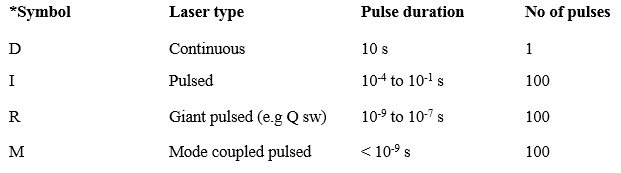
e.g. 532 D LB6 X CE
D = continuous output (see table below)*
532 = offers protection (tested) at a wavelength of 532nm (green)
LB7 = scale number (protection level) 7
X = manufacturer ID
CE = CE Marking (conforms to directive CE 89/686/CEE)
The above example is relatively basic and often the eyewear is tested at several wavelengths. This can result in several lines of detailed markings on the eyewear filters.
|
Revision Questions 1. What are the differences between a class 3B and class 4 laser? 2. Does this laser classification apply to IPL equipment? 3. When purchasing laser eyewear, which 3 variables would you consider? |
Laser Protection Adviser (LPA)
Businesses using lasers may employ the services of a Laser Protection Adviser (LPA). The LPA is a health and safety consultant with expertise in optical radiation safety. The LPA will be able to help assess the risks and recommend appropriate safety controls.
The UK Health and Safety Executive (HSE) have produced a short guidance document, Getting specialist help with health and safety, which sets out a number of criteria that should be considered when choosing a specialist safety consultant (a 'laser protection adviser, LPA' in this context);
- Relevant training, formal qualifications and knowledge,
- Member of a professional body (e.g. IOSH, IIRSM),
- OSHC Registered,
- Adequately insured.
Laser protection supervisor (LPS) / Medical Laser safety officer (MLSO)
Large establishments using lasers may appoint a suitable member of staff to carry out specific duties with respect to laser safety. Traditionally, this involved monitoring that all staff read, understand and sign the laser safety procedures ("local rules").
However, the role of the LPS can be pretty much anything that suits the organisation. In some cases, an LPS is always present to effectively supervise a particular activity. Where the LPS has no management or financial responsibility, it is important to maintain that the overall responsibility for laser safety still lies with the appropriate manager.
In recent years there has been a general move away from extra titles (which can actually cause confusion) in favour of assimilating appropriate duties into those of the responsible manager or existing management structure.
Quality Assurance
It is essential that laser equipment is maintained in good order. This may include,
- Service (by a specialist service engineer)
- Maintenance (routine user checks)
Routine user checks may include,
- Cleaning
- Inspection of fibres/IPL Head
- PPE maintain in good order and cleanliness
- Calibration (if applicable)
- Blinds / Shutters / Interlocks /Warning devices (e.g. illuminated sings) working correctly
Equipment management
For those looking to purchase equipment, problems can be avoided by consideration of the following,
-Service / maintenance provision / Warranty
-Training provision.
-Equipment quality
-Call out times (if there is a problem) /UK based agent
-Compatibility with other equipment and services
-Documentation (manuals, training materials, consultation forms etc.)
-Consumables (e.g. fibres, gels, flash bulbs)
What to do in case of a laser eye injury
If an eye injury is suspected, an ophthalmic examination should be undertaken as soon as possible (nearest A&E hospital) and within 24 hours. This will enable the ophthalmologist to determine what damage has occurred (if any) and that this was due to a recent laser beam strike. Note that damage to the retina is often permanent
|
Revision Questions 1. What is a Laser Protection Adviser (LPA)? 2. What routine safety checks might be useful? 3. What action should you take after a suspected laser eye-strike? |
Medical laser safety management
technical information
Common Machine Variables
Stand by/Ready
In "stand by" mode, the machine is fully powered but the "fire" button/footswitch is disabled. The machine should be placed in ready mode, only when the laser is in place and treatment is about to begin.
Exposure time
The duration of exposure can sometimes be set on laser equipment. This can also be referred to as pulse length or pulse width. For multiple pulse machines, the pulse delay (time between pulses can also be varied)
Energy (radiant energy)
This is basically the amount of light output set. The greater the energy, the greater the heating effect of the beam. This is measured in Joules, J. Sometimes this is expressed as radiant exposure which is the energy per unit area. This is sometimes also defined as "fluence" on some laser equipment, unit: J/cm2
Power (radiant power)
For machines capable of a continuous laser output, the power is the amount of energy per unit time. This is measured in Joules per second, or Watts, W. Again, this can be expressed as power per unit area, or Irradiance (W /m2)
Wavelength
Some laser machines operate at several different wavelengths. Sometimes these are designed to be active all at the same time or on other machines, the wavelength can be selected. For example, many Nd:YAG lasers can be operated at 1064nm, or 532nm. For an IPL, a series of filters are often used to change the spectrum of the output depending upon the treatment.
Repetition frequency
For pulsed lasers, the number of pulsed per unit time can be set. This is typically measured in Hertz (Hz), or pulses per second.
Aiming beam / pilot beam
Many lasers make use of a low power aiming beam of a different colour. Sometimes the intensity of the beam can be varied or the beam can be turned off altogether.
Spot size
In some cases, the focusing or spot size (area of beam at a set distance) of the laser can be varied. In the case of an IPL, different size light guides may be used.
Units
Acronyms